
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.

Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.


Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
For the vast majority of people a scan is unnecessary. For most cases of lower back pain, a comprehensive physiotherapy assessment provides all the information we need to treat your pain effectively.
Imaging of the lower back can sometimes be confusing. We know that many abnormalities seen on scans do not actually cause symptoms, and many people without lower back pain will have similar ‘abnormalities’. One large scientific study found that 50% of people over the age of 30 WITHOUT back pain had disc problems! And that prevalence increased with age. If we treated everyone based solely on what was evident on the scan, the real problem could be missed and hence would not improve. In cases where our examination indicates a serious pathology, we will refer you for a scan and/or to a specialist for further examination.
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
For the vast majority of people a scan is unnecessary. For most cases of lower back pain, a comprehensive physiotherapy assessment provides all the information we need to treat your pain effectively.
Imaging of the lower back can sometimes be confusing. We know that many abnormalities seen on scans do not actually cause symptoms, and many people without lower back pain will have similar ‘abnormalities’. One large scientific study found that 50% of people over the age of 30 WITHOUT back pain had disc problems! And that prevalence increased with age. If we treated everyone based solely on what was evident on the scan, the real problem could be missed and hence would not improve. In cases where our examination indicates a serious pathology, we will refer you for a scan and/or to a specialist for further examination.
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
For the vast majority of people a scan is unnecessary. For most cases of lower back pain, a comprehensive physiotherapy assessment provides all the information we need to treat your pain effectively.
Imaging of the lower back can sometimes be confusing. We know that many abnormalities seen on scans do not actually cause symptoms, and many people without lower back pain will have similar ‘abnormalities’. One large scientific study found that 50% of people over the age of 30 WITHOUT back pain had disc problems! And that prevalence increased with age. If we treated everyone based solely on what was evident on the scan, the real problem could be missed and hence would not improve. In cases where our examination indicates a serious pathology, we will refer you for a scan and/or to a specialist for further examination.
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
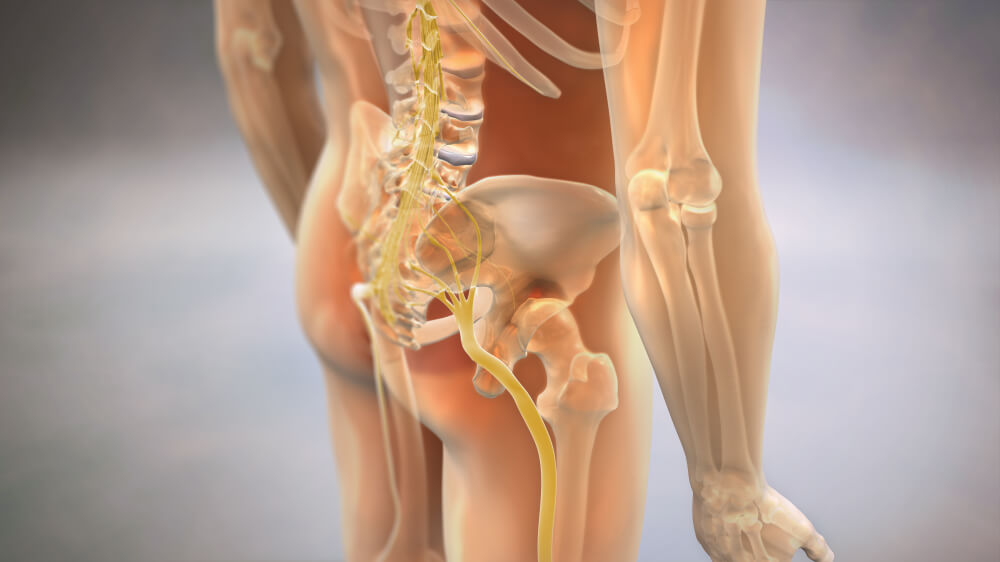
Leg symptoms associated with lower back pain, often referred to as “sciatica”, can be due to either somatic referred pain or radicular referred pain, both of which are described below. Physiotherapists are trained to use specific tests to determine the cause of leg symptoms and treat them appropriately.
For the vast majority of people a scan is unnecessary. For most cases of lower back pain, a comprehensive physiotherapy assessment provides all the information we need to treat your pain effectively.
Imaging of the lower back can sometimes be confusing. We know that many abnormalities seen on scans do not actually cause symptoms, and many people without lower back pain will have similar ‘abnormalities’. One large scientific study found that 50% of people over the age of 30 WITHOUT back pain had disc problems! And that prevalence increased with age. If we treated everyone based solely on what was evident on the scan, the real problem could be missed and hence would not improve. In cases where our examination indicates a serious pathology, we will refer you for a scan and/or to a specialist for further examination.
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
In many cases of lower back pain, it is difficult to identify exactly which structure is causing the pain. During our examination, the first step will be to rule out anything serious.
We will test the spine’s function and decide where there are restrictions in movement or muscle contraction. Back pain is usually caused by a combination of structures and movement patterns rather than one specific joint, disc or muscle. Therefore, trying to pinpoint one specific structure as the cause of the symptoms is often misleading. We base our treatment both on the presenting symptoms as well as movement and activation patterns of the back. We aim to improve function, leading to an immediate reduction in pain and restore normal pain-free movement. There are other factors that are frequently associated with lower back pain, particularly when a person has longstanding or recurrent symptoms.
These may include poor sleep quality, stress, low fitness, problems at work/home or other sicknesses and medical conditions.
These factors can bring on episodes of back pain or increase symptom severity. Physiotherapists understand the complexities of lower back pain and try to address all the contributing factors in our treatment.
Leg symptoms associated with lower back pain, often referred to as “sciatica”, can be due to either somatic referred pain or radicular referred pain, both of which are described below. Physiotherapists are trained to use specific tests to determine the cause of leg symptoms and treat them appropriately.
For the vast majority of people a scan is unnecessary. For most cases of lower back pain, a comprehensive physiotherapy assessment provides all the information we need to treat your pain effectively.
Imaging of the lower back can sometimes be confusing. We know that many abnormalities seen on scans do not actually cause symptoms, and many people without lower back pain will have similar ‘abnormalities’. One large scientific study found that 50% of people over the age of 30 WITHOUT back pain had disc problems! And that prevalence increased with age. If we treated everyone based solely on what was evident on the scan, the real problem could be missed and hence would not improve. In cases where our examination indicates a serious pathology, we will refer you for a scan and/or to a specialist for further examination.
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
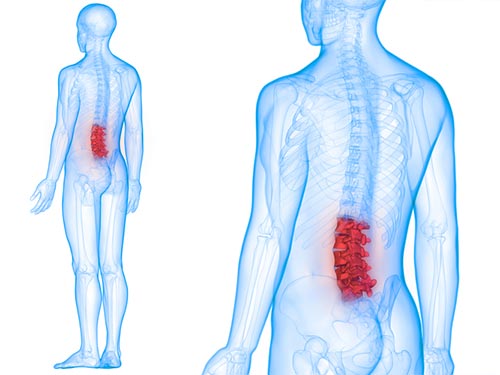
The lower back or “lumbar spine”, consists of 5 vertebrae (bones) in the lowest part of the spine. Lower back pain is a common condition that most of us will experience at some stage in our lives.
There are several different causes of lower back pain, with the vast majority of cases being of musculoskeletal origin without any serious structural damage. These cases respond very well to physiotherapy, which will usually include manual therapy, exercises and activity/postural modifications.
Very rarely, a person’s lower back pain may be a symptom of a more serious underlying problem. In such cases, a physiotherapist is able to assess the problem and refer to the correct medical practitioner for appropriate care.
In many cases of lower back pain, it is difficult to identify exactly which structure is causing the pain. During our examination, the first step will be to rule out anything serious.
We will test the spine’s function and decide where there are restrictions in movement or muscle contraction. Back pain is usually caused by a combination of structures and movement patterns rather than one specific joint, disc or muscle. Therefore, trying to pinpoint one specific structure as the cause of the symptoms is often misleading. We base our treatment both on the presenting symptoms as well as movement and activation patterns of the back. We aim to improve function, leading to an immediate reduction in pain and restore normal pain-free movement. There are other factors that are frequently associated with lower back pain, particularly when a person has longstanding or recurrent symptoms.
These may include poor sleep quality, stress, low fitness, problems at work/home or other sicknesses and medical conditions.
These factors can bring on episodes of back pain or increase symptom severity. Physiotherapists understand the complexities of lower back pain and try to address all the contributing factors in our treatment.
Leg symptoms associated with lower back pain, often referred to as “sciatica”, can be due to either somatic referred pain or radicular referred pain, both of which are described below. Physiotherapists are trained to use specific tests to determine the cause of leg symptoms and treat them appropriately.
For the vast majority of people a scan is unnecessary. For most cases of lower back pain, a comprehensive physiotherapy assessment provides all the information we need to treat your pain effectively.
Imaging of the lower back can sometimes be confusing. We know that many abnormalities seen on scans do not actually cause symptoms, and many people without lower back pain will have similar ‘abnormalities’. One large scientific study found that 50% of people over the age of 30 WITHOUT back pain had disc problems! And that prevalence increased with age. If we treated everyone based solely on what was evident on the scan, the real problem could be missed and hence would not improve. In cases where our examination indicates a serious pathology, we will refer you for a scan and/or to a specialist for further examination.
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.
Lower back pain is one of the leading causes of pain and disability around the world. Physiotherapy is very effective at managing the pain and dysfunction associated with problems in this area. Read on to see answers to a number of common questions and how physiotherapy can help you.
The lower back or “lumbar spine”, consists of 5 vertebrae (bones) in the lowest part of the spine. Lower back pain is a common condition that most of us will experience at some stage in our lives.
There are several different causes of lower back pain, with the vast majority of cases being of musculoskeletal origin without any serious structural damage. These cases respond very well to physiotherapy, which will usually include manual therapy, exercises and activity/postural modifications.
Very rarely, a person’s lower back pain may be a symptom of a more serious underlying problem. In such cases, a physiotherapist is able to assess the problem and refer to the correct medical practitioner for appropriate care.
In many cases of lower back pain, it is difficult to identify exactly which structure is causing the pain. During our examination, the first step will be to rule out anything serious.
We will test the spine’s function and decide where there are restrictions in movement or muscle contraction. Back pain is usually caused by a combination of structures and movement patterns rather than one specific joint, disc or muscle. Therefore, trying to pinpoint one specific structure as the cause of the symptoms is often misleading. We base our treatment both on the presenting symptoms as well as movement and activation patterns of the back. We aim to improve function, leading to an immediate reduction in pain and restore normal pain-free movement. There are other factors that are frequently associated with lower back pain, particularly when a person has longstanding or recurrent symptoms.
These may include poor sleep quality, stress, low fitness, problems at work/home or other sicknesses and medical conditions.
These factors can bring on episodes of back pain or increase symptom severity. Physiotherapists understand the complexities of lower back pain and try to address all the contributing factors in our treatment.
Leg symptoms associated with lower back pain, often referred to as “sciatica”, can be due to either somatic referred pain or radicular referred pain, both of which are described below. Physiotherapists are trained to use specific tests to determine the cause of leg symptoms and treat them appropriately.
For the vast majority of people a scan is unnecessary. For most cases of lower back pain, a comprehensive physiotherapy assessment provides all the information we need to treat your pain effectively.
Imaging of the lower back can sometimes be confusing. We know that many abnormalities seen on scans do not actually cause symptoms, and many people without lower back pain will have similar ‘abnormalities’. One large scientific study found that 50% of people over the age of 30 WITHOUT back pain had disc problems! And that prevalence increased with age. If we treated everyone based solely on what was evident on the scan, the real problem could be missed and hence would not improve. In cases where our examination indicates a serious pathology, we will refer you for a scan and/or to a specialist for further examination.
Physiotherapy is one of the most effective methods for the treatment of lower back pain. There is a large amount of research to support the techniques that we use. Most cases of lower back pain respond well to a program of manual therapy and graded exercises. Manual therapy can include massage, and joint mobilisations and manipulations. These techniques reduce pain and help to restore movement. The exercise program typically includes a combination of range of motion and mobility exercises, trunk and leg strengthening exercises, and a gradual return to activities. Physiotherapists can also use other forms of treatment such as acupuncture, taping and TENS.
Activity modification: limit exposure to symptom provoking activity.
The primary goal of initial injury management is to manage symptoms. This may include avoidance of rapid movements, heavy lifting or dynamic/uncontrolled situations.
If you are an athlete, other options may include reducing overall workload or intensity of exercise, and limiting range of motion.
Oftentimes, athlete may become fear avoidant of performing a movement similar to the one that caused the injury. This, other goals may include improving confidence with movement. This can be achieved by the above mentioned recommendations.